How to Read an Mri Report for Shoulder
OVERVIEW
This chapter is an outline of the basic principles of magnetic resonance imaging (MRI) of the shoulder with an emphasis on the clinical issues related to the imaging findings of shoulder pathology. The radiologic technique for shoulder imaging and basic shoulder beefcake are start discussed. An outline of common pathologic processes of impingement and instability follows. Next, there is a depiction of the disease processes of "dead arm," acromioclavicular separation, and pectoralis major rupture. Then there is a discussion of tenosynovitis, arthritis, neoplasia, and avascular necrosis. Lastly, at that place is a synoptic discussion of mutual surgical procedures for impingement and instability along with common operative and postoperative complications of these techniques.
RADIOLOGIC TECHNIQUE
Technique for assessment of shoulder pathology differs amid institutions based on radiologists' preferences. A few general comments about conventional and arthrographic MRI protocols will be made.
The shoulder in a conventional MRI examination is acquired in partial external rotation in the centric, coronal and sagittal planes. Confirmation of pathology in different planes and sequences increases diagnostic accuracy. The coronal aeroplane is acquired along the long axis of the supraspinatus tendon. The sagittal plane is acquired parallel to the glenoid articular surface and perpendicular to the long axis of the supraspinatus. Other views such as abduction and external rotation (ABER) in the coronal plane may be obtained equally role of a conventional or arthrographic exam.one The anterior band of junior glenohumeral ligament is optimally depicted on the abduction external rotation view, as it is under tension. The abduction external rotation view of the shoulder is helpful in demonstrating subtle anterior inferior labral tears, partial articular surface rotator gage tears, and instability of the shoulder in ABER.
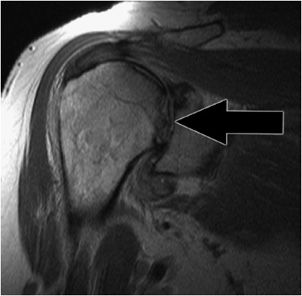
Sequences may be tailored according to clinical indication. MRI shoulder protocols typically involve fat-saturated proton density images that are sensitive to internal derangement. T2 star gradient recall echo images are employed in the assessment of the labrum and for detection of substances that produce susceptibility effects such equally calcium hydroxyapatite or loose surgical hardware. T1-weighted images are useful for the assessment of bone marrow derangement or rotator cuff atrophy (Figure 12-i). Non-fatty-saturated T2-weighted images are useful in characterizing tendon pathology, particularly discerning tendinosis from tear (Figure 12-two).
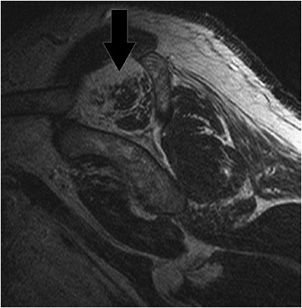
Figure 12-one. Chronic muscle atrophy. T1-weighted sagittal epitome optimally depicts advanced musculus atrophy and fatty degeneration around the shoulder including the supraspinatus (black arrow).
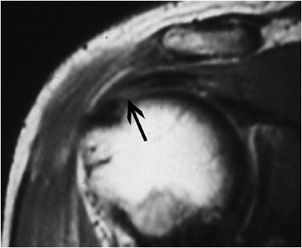
Effigy 12-two. Tendinosis of the supraspinatus tendon. Coronal oblique T2-weighted image shows intermediate signal in the tendon indicating tendinosis.
MR arthrography is employed for the detection of subtle rotator cuff tears or labral pathology in patients with a negative conventional MRI, the assessment of the postoperative shoulder, and the demonstration of communication between the joint and extra-articular pathology such as a paralabral cyst.ii Direct MR arthrography distends the articulation through the percutaneous injection of a diluted gadolinium solution. Nether fluoroscopic guidance, nigh 12 cc of a 1:200 gadolinium dilution solution is injected into the glenohumeral joint prior to imaging. T1 fat-suppressed images in the three conventional planes and ABER view are obtained along with a T2-weighted sequence without fatty suppression. The T2-weighted sequence is necessary to distinguish between pathologic fluid collections such as a bursa or cyst and the injected intra-articular contrast. Complications of direct arthrography are rare. These include synovitis, bleeding, infection, or an allergic reaction. Less commonly indirect or intravenous arthrography may be performed with an injection of gadolinium at the standard intravenous dose 10–20 minutes prior to imaging. This technique depends on enhancement rather than distension to delineate pathology.
BASIC SHOULDER Anatomy
The shoulder consists of the clavicle, scapula, and humeral caput. Information technology consists of four joints: sternoclavicular, acromioclavicular, scapulothoracic, and glenohumeral.
The shoulder is the most mobile joint in the body. The boggling range of the shoulder is due to the shallow osseous glenohumeral articulation. The stability of the shoulder is maintained by static and dynamic stabilizers: principally the rotator cuff, the long head of the biceps tendon, the glenoid labrum, the joint capsule, and the coracoacromial curvation.
The rotator gage muscles are dynamic stabilizers of the glenohumeral joint. They originate around the scapula and attach to the humeral head. The subscapularis is the anterior rotator gage muscle. Information technology originates from the subscapular fossa of the scapula and attaches to the lesser tuberosity of the proximal humerus. It internally rotates and adducts the arm. The supraspinatus is the superior rotator cuff muscle. It originates in the supraspinatus fossa (superior to the scapular spine) and attaches to the almost superior aspect of the greater tuberosity. Its principal action is abduction. The infraspinatus and teres minor are posterior rotator cuff muscles. The infraspinatus arises from the infraspinous fossa. The teres minor originates at the lateral border of the scapula inferior to the infraspinatus. The infraspinatus and teres modest also attach to the greater tuberosity, superiorly and inferiorly, respectively. The infra-spinatus externally rotates the arm. The teres minor is an external rotator and adductor of the arm. The subscapularis is innervated by the subscapular nerve. The supraspinatus and infraspinatus are innervated past the suprascapular nervus that passes through the suprascapular and spinoglenoid notches, mutual sites of entrapment. The teres minor and deltoid are innervated past the axillary nerve. The axillary nerve passes through the quadrilateral infinite (jump by the two teres muscles, long head of the triceps and humeral shaft). The infinite betwixt the supraspinatus and subscapularis is the rotator interval that contains the coracohumeral and superior glenohumeral ligaments and long head of the biceps tendon. The rotator interval narrows laterally and ends at the supraspinatus and subscapularis insertion.
The long head of the biceps tendon is a dynamic stabilizer of the glenohumeral joint. The tendon has intra-articular and extra-articular components. The long head of the biceps originates at the supraglenoid tubercle and spans the rotator interval and intertubercular groove. In the rotator interval, the long head of the biceps is stabilized by a pulley mechanism consisting of the coracohumeral ligament (which also resists posterior junior translation) and superior glenohumeral ligament. A secondary stabilizer of the long head of the biceps is the transverse ligament or distal zipper of the subscapularis tendon in the proximal intertubercular groove. The long head of the biceps prevents inductive superior translation of the humeral head. The short head of the biceps arises along with the coracobrachialis from the coracoid process. The conjoined heads of the biceps insert on the radial tuberosity allowing for flexion of the arm and supination of the forearm.
The articulation sheathing is a static stabilizer of the glenohumeral joint. Thickenings of the joint capsule are described as the superior, middle, and junior glenohumeral ligaments. The superior glenohumeral ligament (as part of the biceps pulley forth with the coracohumeral ligament) is important in stabilization of the long head of the biceps tendon. Information technology originates anterior to the long head biceps origin and inserts with the coracohumeral ligament to the bottom tuberosity. The middle glenohumeral ligament (Figure 12-3) is most hands appreciated deep to the subscapularis tendon. The junior glenohumeral ligament is shown along the inferior aspect of the glenohumeral joint. The junior glenohumeral ligament consists of inductive and posterior bands with an intervening axillary pouch, the most dependent portion of the articulation. Normal outpouchings of the joint capsule include the biceps tendon sheath, axillary recess, rotator interval, and subscapularis recess.
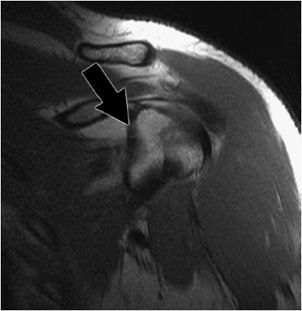
Figure 12-3. Center glenohumeral ligament. Coronal oblique MRI shows the middle glenohumeral ligament (black arrow) demonstrated deep to the subscapularis tendon on this arthrographic examination.
The glenoid labrum is a static stabilizer of the glenohumeral joint. It is a fibrocartilaginous structure that deepens the shallow normally anteverted glenoid cavity. The anterior labrum is normally larger than the posterior. Variations in labral attachment and congenital deficiency may be confused with pathology. These include the sublabral recess, sublabral foramen, and the Buford complex. A sublabral recess is a smoothly tapered fractional detachment of the superior labrum from the underlying glenoid. A sublabral foramen is a complete disengagement of the inductive superior labrum that reattaches inductive inferiorly. The Buford circuitous is absenteeism or hypoplasia of the anterior superior labrum associated with a thickened middle glenohumeral ligament. Lesions of the labrum may be localized past quadrants or in terms of a clockface position. For example, a two o'clock lesion is localized to the anterior superior quadrant.
The coracoacromial arch is a static stabilizer of the anterior superior aspect of the glenohumeral articulation. Information technology consists of the coracoid process, coracoacromial ligament, and acromion. The arch stabilizes the humeral head preventing its superior subluxation. Narrowing of the acromiohumeral interval due to abnormalities of the components of the arch in the setting of subacromial impingement may shrink the subacromial/subdeltoid bursa or rotator gage.
IMPINGEMENT
Impingement is the abnormal compression of structures associated with a joint due to congenital or acquired structural abnormalities or due to joint instability. Impingement is a clinical diagnosis that may be supported with radiologic findings.3
Impingement may be classified every bit external or internal and primary or secondary. External impingement involves compression of the external or extra-articular aspect of the joint, for case, the bursal surface of the rotator cuff. Internal impingement involves compression of the intra-articular aspect of the joint, for example, the labrum or articular surface of the rotator gage.4 Master impingement is due to structural abnormalities of the coracoacromial arch. Secondary impingement is due to instability of the articulation.
Subacromial and subcoracoid external impingement will be discussed. Then anterior superior and posterior superior internal impingement will exist outlined.
The classic form of shoulder impingement is subacromial that may be primary due to built or acquired structural causes or secondary due to joint instability (discussed in the adjacent department). Subacromial impingement is elicited in flexion or abduction. Patients with shoulder impingement typically present with activity-related diffuse pain in the region of the deltoid muscle. The pain is worst at night.
Structural causes for subacromial impingement are due to coracoacromial curvation abnormalities: the shape and slope of the acromion, an os acromiale, coracoacromial ligament thickening, or acromioclavicular separation.
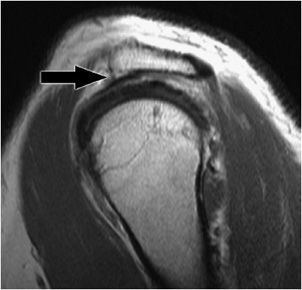
The shape of the undersurface of the acromion may be classified according to morphology: type one (Effigy 12-4), apartment undersurface; type 2, concave undersurface (Effigy 12-v); type 3, acromion, anterior lateral hook (Figure 12-6). Anterior or lateral downsloping of the acromion may narrow the acromiohumeral interval and predispose patients to impingement.
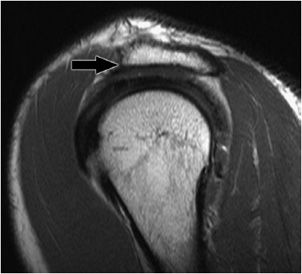
Figure 12-iv. Blazon 1 acromion. Sagittal MRI shows flat undersurface of the inductive lateral acromion consequent with type one acromion (black arrow).
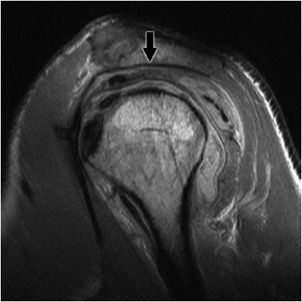
Figure 12-v. Type 2 acromion. Sagittal MRI shows concave undersurface of the acromion consequent with type 2 acromion (black arrow). Underlying subacromial/subdeltoid bursitis and rotator cuff tendinopathy are also demonstrated.
Effigy 12-6. Type 3 acromion. Sagittal MRI shows a claw of the anterior lateral acromion (black pointer) consistent with a type 3 acromion. This acromial morphology has been associated with subacromial impingement.
An os acromiale (Figure 12-7) is an unfused acromial ossification center. It may crusade clinical impingement that is thought to exist due to downward traction of the ossification middle with contraction of the deltoid muscle.
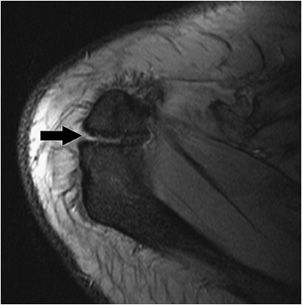
Figure 12-7. Os acromiale. Axial MRI shows a synchondrosis (black pointer) of the unfused os acromiale. This finding has been associated with subacromial impingement.
Thickening of the coracoacromial ligament every bit part of the coracoacromial arch may cause stenosis of the acromiohumeral interval. Coracoacromial ligament resection is part of the subacromial decompression operation. This structure should non be resected if at that place is an irreparable rotator cuff tear, as it resists anterior superior humeral caput escape.
Subacromial impingement is initially associated with subacromial/subdeltoid bursitis (Figure 12-viii). As impingement evolves, tendinosis develops in the bursal aspect of the supraspinatus. Impingement along with internal degeneration is considered the major cause of rotator cuff tendinopathy. Tendinosis presents as thickening of and aberrant bespeak in the tendon. Progression of the process leads to partial tears or discontinuity of the tendon and eventually full-thickness rotator cuff tears (Figures 12-9 to 12-11). A full-thickness rotator gage tear represents a defect that allows communication between the bursal and articular aspects of the cuff. A full-thickness tear may progress to a consummate tear. A complete tear (Figures 12-12 and 12-13) is full discontinuity of the tendon that is frequently associated with superior migration of the humeral caput. Chronic repetitive trauma of the superiorly subluxed humeral caput may lead to remodeling of the acromion and eventual collapse of the humeral head (rotator gage arthropathy).
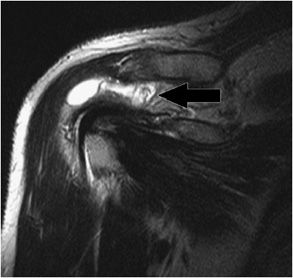
Figure 12-8. Subacromial/subdeltoid bursitis. Coronal oblique MRI shows fluid and synovitis (black arrow) in the subacromial/subdeltoid bursa consistent with avant-garde bursitis. These findings might exist associated with subacromial impingement or inflammatory arthritis.
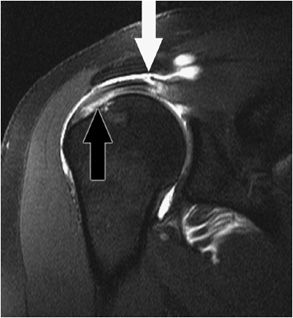
Figure 12-ix. Bursal and articular surface rotator gage tears. Coronal oblique MRI shows a disruption of the articular surface of the supraspinatus near its insertion (black arrow). There is a bursal surface tear of the supraspinatus near the myotendinous junction (white arrow).
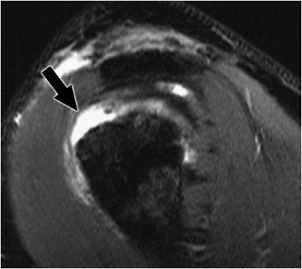
Effigy 12-10. Full-thickness rotator gage tear. Sagittal fat-saturated MRI of the shoulder shows a gap in the anterior aspect of the supraspinatus that traverses the entire width of the tendon from the bursal to the articular surface (black arrow) consequent with a full-thickness tear. The posterior supraspinatus fibers are intact.
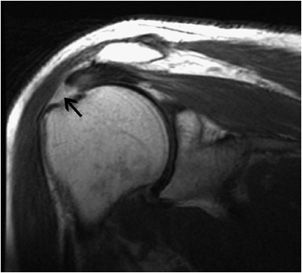
Effigy 12-xi. Full-thickness tear of the supraspinatus at the insertion site. Coronal oblique spin echo T2-weighted image shows fluid signal (black arrow) in the insertion of the supraspinatus without retraction of tendon indicating total-thickness tear.

Figure 12-12. Complete rotator gage tear. Sagittal MRI shows there is a gap that involves the entire supraspinatus tendon (black pointer) in this patient who is condition post rotator gage repair. These findings are consequent with compete retear of the supraspinatus. Note vivid signal fluid is replacing the torn tendon.
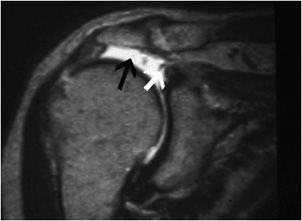
Figure 12-thirteen. Complete tear of the supraspinatus at the insertion site. Coronal oblique MRI shows bright fluid signal replacing the completely torn supraspinatus tendon (black pointer). Note the white arrow is pointing to torn and retracted supraspinatus tendon.
A description of a rotator gage tear should include the portion of the tendon involved (articular, intrasubstance, or bursal); location/size/shape of the defect; and any associated musculus volume loss/fat degeneration, tendon retraction, or extension into the rotator interval.5 The size of full-thickness defects is given in ii dimensions. The depth of partial thickness tears is estimated based on a normal thickness of approximately 1.2 cm. The morphology of the tear may be described as crescentic (mild medial retraction), U-shaped (massive tear involving the inductive posterior dimension of the gage), and L-shaped (massive tear with preservation of the anterior cuff). The determination to repair a cuff tear may be based on prognostic imaging findings, symptoms, and functional expectations of the patient.
Subcoracoid external impingement is associated with a narrowing of the coracohumeral interval to less than 7 mm. The narrowed interval is thought to facilitate impingement of the distal subscapularis tendon and its overlying subcoracoid and anterior subdeltoid bursae. Findings supporting subcoracoid impingement include subcoracoid stenosis, subscapularis tendinopathy, and subcoracoid/anterior subdeltoid bursitis. Patients with anterior superior instability due to a biceps pulley injury are predisposed to secondary subcoracoid impingement due to abnormal anterior superior translation of the humeral head.
Anterior superior internal impingement is an uncommon diagnosis due to biceps pulley injury. This entity is referred to every bit the "hidden lesion" due to the difficulty of making the diagnosis based on clinical or arthroscopic findings. The biceps pulley stabilizes the long head of the biceps tendon that is a chief restraint to inductive superior subluxation of the humeral head. Disruption of the biceps pulley may be due to degeneration, acute trauma, or repetitive micro-trauma.6 During adduction and internal rotation, insufficiency of the biceps pulley allows for impingement of the anterior supraspinatus, superior subscapularis tendons, and anterior superior labrum due to compression past the anteriorly/superiorly translated humeral head. This grade of impingement is associated with the complex of lesions classified by the term "microinstability." These include the superior labral inductive cuff (SLAC) tear lesion.
Posterior superior internal impingement is frequently seen in patients who engage in repetitive overhead able-bodied activities. There is normal contact between the humeral head and the posterior superior corner of the glenohumeral joint in ABER. Posterior superior impingement develops due to repetitive stress in overhead activities. It is associated with lesions of the superior labrum, posterior supraspinatus, and superior infraspinatus.
INSTABILITY
Patients with instability present with hurting and apprehension with ABER and are prone to recurrent subluxation and dislocation. Instability may be due to insufficiency of any of the static or dynamic stabilizers of the glenohumeral joint secondary to a traumatic issue, the repetitive microtrauma of impingement, or congenital capsular laxity.7
First, there is a discussion of posttraumatic anterior glenohumeral instability. Then microinstability (microtraumatic instability) volition be defined and the associated lesions of superior labral anterior to posterior (SLAP) and SLAC tears will be outlined. Finally, multidirectional instability will exist discussed.
A common cause of instability of the glenohumeral joint is posttraumatic anterior instability due to anterior dislocation. Anterior dislocation of the shoulder is associated with injury to the inductive inferior labrum or osseous glenoid rim with an associated defect in the posterolateral aspect of the humeral head articular surface. These lesions are described respectively as Bankart/Bankart variant and Loma–Sachs lesions (Figures 12-xiv to 12-xvi). An osseous Bankart lesion involves the anterior ring of the inferior glenohumeral ligament, the anterior inferior labrum, the adjacent medial scapular periosteum, and the underlying osseous glenoid rim. A nonosseous Bankart spares the bony glenoid rim. Injuries of the posterior inferior glenoid associated with posterior dislocation are called reverse Bankart lesions (Figure 12-17).
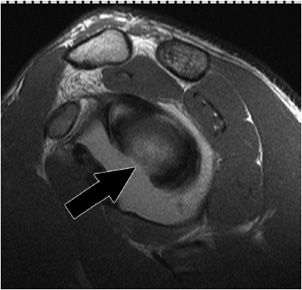
Figure 12-fourteen. Osseous Bankart. Sagittal MRI shows a defect in the inductive junior aspect of the glenoid (black arrow) consequent with osseous Bankart lesions related to an anterior dislocation.
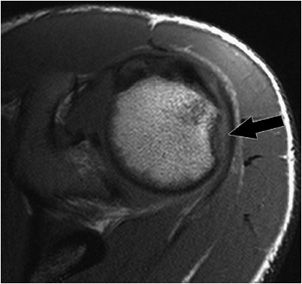
Figure 12-xv. Hills–Sachs lesion. There is a small osseous defect of the posterior lateral humeral head (blackness arrow) consistent with a Hill–Sachs lesion related to a remote anterior dislocation.
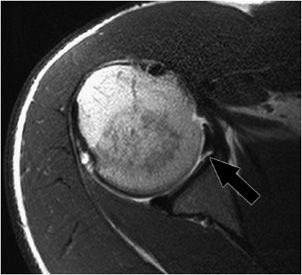
Effigy 12-xvi. Anterior junior labral tear. Axial MRI shows in that location is a tear of the anterior inferior aspect of the labrum (black arrow) consequent with a nonosseous Bankart lesion.
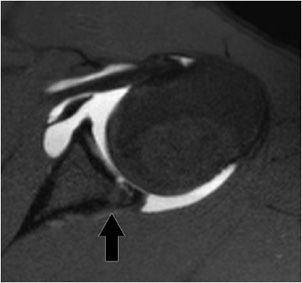
Figure 12-17. Reverse Bankart lesion. Axial MRI shows there is an osseous reverse Bankart lesion (black arrow) with disruption of the posterior inferior labrum and a fracture of the posterior inferior osseous glenoid rim. Note a modest articular cartilage defect representing GLAD lesion.
A diverseness of anterior labroligamentous circuitous/Bankart variant injuries have been described (Figure 12-xviii).8 The inductive labroligamentous periosteal sleeve avulsion (ALPSA) lesion is characterized by an intact medial scapular periosteum against which the torn labroligamentous circuitous migrates. A Perthes lesion is nondisplaced anterior inferior labral disruption that may simply be seen on the abduction external rotation view (Figure 12-19). A glenolabral articular disruption (GLAD) lesion is a nondisplaced anterior inferior labral tear with next chondral injury. A lateral tear of the inductive capsule, so-called humeral avulsion of the glenohumeral ligament (HAGL) lesion, may occur with anterior dislocation and may be associated with posttraumatic anterior instability.
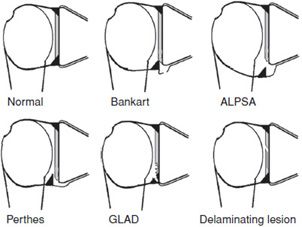
Figure 12-eighteen. Labral and cartilage lesions of the glenoid.

Figure 12-nineteen. Perthes on ABER. ABER view for MRI shows there is a tear of the anterior inferior labrum that could only exist appreciated on the ABER view consistent with a nondisplaced Perthes type tear (black pointer). Contrast extravasation from the arthrogram procedure is also demonstrated.
Microinstability (microtraumatic instability) is a full general expression for lesions of the superior one-half of the glenohumeral joint. These lesions are commonly due to repetitive overhead action or a fall on an outstretched hand (FOOSH) injury. Two characteristic forms of microtraumatic instability volition be discussed. Beginning, SLAP lesions will be outlined. Then, SLAC lesions volition be delineated.
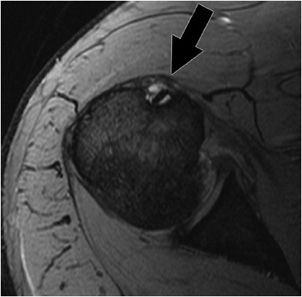
SLAP tears (Figure 12-20) are mutual injuries in athletes. They are staged into several types according to morphology (fraying, avulsion, bucket handle tear) and the extent of the interest of the labrum, biceps anchor, or sheathing. Labral tears may exist associated with paralabral cysts. These cysts may extend from the site of the tear and crusade nervus entrapment. Paralabral cysts in the suprascapular notch are associated with entrapment of the suprascapular nerve fibers innervating the supraspinatus and infraspinatus; cyst extension into the spinoglenoid notch may cause isolated infraspinatus denervation (Effigy 12-21). Paralabral cysts may extend into the quadrilateral space demarcated by the teres minor, teres major, humeral shaft, and long head of the triceps. Quadrilateral space pinch is associated with axillary nerve entrapment and deltoid/teres minor denervation. Treatment of these lesions requires decompression of the mass effect on the entrapped nerve.
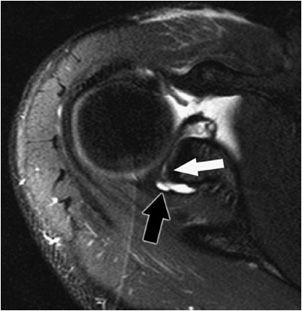
Figure 12-20. SLAP tear. Centric MRI shows paralabral cysts (black pointer) associated with a superior labral anterior to posterior tear. Paralabral cysts might be associated with nerve entrapment and denervation of rotator gage muscles.
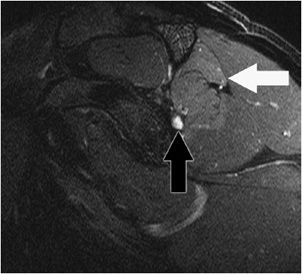
Figure 12-21. Infraspinatus denervation. Sagittal MRI shows a small paralabral cyst (black arrow) in the region of the supraglenoid notch associated with denervation changes in the infraspinatus tendon (brighter than normal betoken in the muscle) likely due to pinch of the infraspinatus branch of the suprascapular nerve.
SLAC tears are associated with anterior superior instability. Disruption of the biceps pulley mechanism predisposes to aberrant translation of the humeral caput. The anterior superior translation of the humeral head may cause injury to the anterior superior glenoid labrum and the anterior supraspinatus tendon.
Multidirectional instability is defined every bit current subluxation or dislocation of the glenohumeral articulation in more than than one direction. This condition is multifactorial due to capsular insufficiency that may exist secondary to congenital laxity, a pregnant traumatic upshot, or repetitive microtraumatic events. The MRI findings associated with multidirectional instability are enlargement of the inferior pouch and the rotator interval. Patients with atraumatic multidirectional instability often undergo rehabilitation or surgical treatment such every bit inferior capsular shift.
"Dead ARM"
"Dead arm" is a condition characterized by the sudden loss of the ability to throw a fastball in the elite overhead athlete.9,ten The result immediately preceding this condition is a posterior SLAP 2 tear. The throwing mechanism consists of phases described as wind upwardly, early cocking, tardily cocking/early acceleration, late acceleration, and follow-through (deceleration). In the follow-through phase of the throwing mechanism, at that place is maximal stress on the posterior inferior capsule. In the elite overhead athlete, repetitive loading of the posterior capsule causes pathologic tightening of the posterior band of the junior glenohumeral ligament (associated with glenohumeral internal rotation arrears (GIRD) and mineralization of the posterior band described as the Bennett lesion). In the late cocking/early dispatch phase of the throwing mechanism, the arm is in maximal ABER. In ABER, the thickened posterior band of the inferior glenohumeral ligament acts as a sling that causes forceful clearance of the greater tuberosity. The normal contact between the greater tuberosity and the posterior superior corner of the glenoid in ABER is prevented by the clearance of the greater tuberosity past the thickened posterior capsule. The clearance of the greater tuberosity allows for abnormally increased external rotation that stresses the posterior superior corner of the joint. The abnormal stress is associated with lesions of the superior labrum, posterior supraspinatus, and superior infraspinatus. Furthermore, there is fatigue of the rotator gage musculature. Fatigue of the rotator cuff muscles due to abnormally increased external rotation is associated with the scapular malposition, inferior medial edge prominence, coracoid pain, dyskinesis of scapular motility (SICK) scapula. The Sick scapula is in abduction and protraction. Tension on the superior and medial scapula by the levator scapulae causes a painful tendinopathy.
ACROMIOCLAVICULAR SEPARATION
The acromioclavicular joint (ACJ) is stabilized by the conoid and trapezoid portions of the coracoclavicular (CC) ligaments. The clavicle is further stabilized by the trapezius and deltoid that attach to the clavicle, acromion, and spine of scapula, posteriorly and anterolaterally, respectively. Acromioclavicular separation (Figure 12-22) may occur after a direct fall onto the shoulder. MRI tin assist in identifying and grading these injuries.11 Six grades of acromioclavicular separation are described under the Rockwood classification. Grade 1 acromioclavicular separation represents a sprain of the ACJ that manifests as edema on the MRI examination. Grade 2 separation is disruption of the ACJ with intact CC ligaments. Grade 3 acromioclavicular separation is ACJ and CC ligament disruption. Course 4 separation is ACJ and CC ligament disruption along with posterior displacement of the clavicle that may disrupt fibers of the trapezius. Form 5 separations ACJ and CC ligament disruption along with tears of the deltoid and trapezius associated with superior displacement of the clavicle. Grade 6 separation differs from grade 5 injuries as the clavicle is inferiorly displaced.

Effigy 12-22. Acromioclavicular separation. Coronal oblique MRI shows tears of the coracoclavicular ligaments (white arrow) and disruption and malalignment of the acromioclavicular articulation (blackness arrow). These findings are consequent with type iii acromioclavicular separation.
PECTORALIS MAJOR RUPTURE
Sternal and clavicular fibers constitute the pectoralis major muscle. The ii components adhere to the lateral aspect of the bicipital groove of the proximal humerus. The muscle is an internal rotator, flexor, and adductor of the arm. Amongst weight lifters, this lesion is commonly associated with bench printing injury. Most injuries involve both components at the myotendinous junction. Yet, the unabridged muscle including the origin, belly, myotendinous junction, and tendon should be interrogated on coronal and axial images (Effigy 12-23).
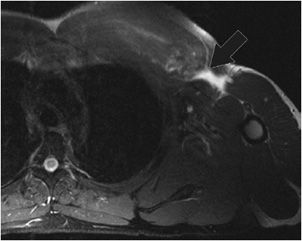
Figure 12-23. Pectoralis major rupture. Centric MRI shows a gap in the expected location of the pectoralis major tendon consistent with a tear (black arrow).
BICEPS TENOSYNOVITIS/TENDINOPATHY
Long caput of the biceps tenosynovitis may be associated with repetitive stress/microtrauma. It is often associated with shoulder impingement. In the absenteeism of a joint effusion, fluid or synovitis in the biceps sheath is suggestive of biceps tenosynovitis (Figure 12-24). Biceps tendinopathy may be treated with tenodesis (resection and reattachment of the biceps to the bicipital groove) or tenotomy (resection of the tendon assuasive release of tendon with distal retraction).
Effigy 12-24. Tenosynovitis. Axial MRI shows fluid and synovitis around the long head of the biceps tendon in the bicipital groove consequent with tenosynovitis (black arrow).
ARTHRITIS
Osteoarthritis of the glenohumeral and ACJs manifests in the same way equally the weight-bearing joints. Considering the glenohumeral articulation non a weight-bearing joint, de novo osteoarthritis is less common, and posttraumatic versus calcium pyrophosphate deposition disease (CPPD) should exist considered in cases of astringent osteoarthritis of the shoulder. In the glenohumeral joint, there is disproportionate loss of cartilage unduly involving the posterior glenoid rim. As the illness progresses, in that location is formation of osteophytes, subchondral sclerosis/cyst germination, and synovitis (Effigy 12-25). In the ACJ, capsular hypertrophy may exist a prominent finding. Although acromioclavicular osteoarthritis is common, subchondral edema is associated with symptomatic cases presenting as anterior superior pain. Conservative treatment of osteoarthritis includes anti-inflammatory drugs and physical therapy. Advanced glenohumeral arthritis is treated with arthroplasty. Distal clavicular resection (Mumford procedure) is undertaken in avant-garde cases of acromioclavicular arthritis.

Figure 12-25. Avant-garde osteoarthritis. Coronal oblique MRI shows a total-thickness chondral loss of the glenoid articular surface (black pointer). At that place is synovitis in the axillary pouch (white arrow). Subchondral cysts and osteophytes are demonstrated in this case of severe osteoarthritis of the glenohumeral joint.
Rheumatoid arthritis is a systemic inflammatory process of uncertain etiology that results in synovial inflammation. It may affect the shoulder manifesting with synovitis, erosions, and rotator cuff tears. In contradistinction to degenerative osteoarthritis, cartilage loss is seen in a more compatible distribution and marginal erosions are characteristic.
Other inflammatory conditions such as calcium hydroxyapatite deposition illness (HADD) may affect the shoulder (Figure 12-26). Calcium deposition can be seen in the rotator cuff, bursae, or in the tissues around the joint. The deposits may exist asymptomatic or cause mechanical or inflammatory symptoms.
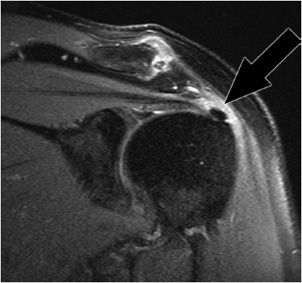
Figure 12-26. Calcific tendinitis. Coronal oblique MRI shows calcium hydroxyapatite deposition in the supraspinatus at its insertion on the footprint is associated with mild side by side edema (black arrow).
NEOPLASIA
Neoplastic conditions of the shoulder are rare. Common benign tumors involving the shoulder include enchondromas and osteochondromas (Effigy 12-27). Metastatic affliction to the shoulder is a more than common entity in elderly patients. Multiple myeloma, chondrosarcoma, and Ewing sarcoma (Effigy 12-28) are some of the more common primary malignancies affecting the shoulder region.
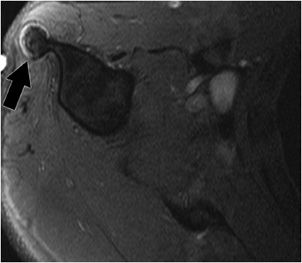
Figure 12-27. Osteochondroma. Axial MRI shows a chondral cap of an osteochondroma (black pointer) arising from the humeral shaft. Continuity of the marrow of the exostosis with the central marrow crenel of the humerus is essential in the diagnosis.
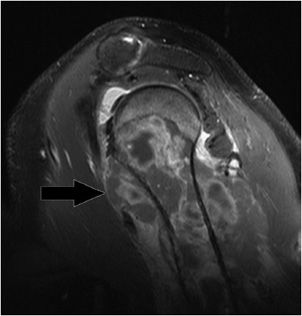
Figure 12-28. Ewing sarcoma. Sagittal MRI shows an ambitious soft tissue component of Ewing sarcoma that has infiltrated the diaphysis and metaphysis of the proximal humerus (black arrow). Note inhomogeneous point intensities in the humerus and surrounding soft tissue.
AVASCULAR NECROSIS
Avascular necrosis of the shoulder is often asymptomatic or presents with generalized hurting. Information technology is less common than in the hip. This condition may be secondary to traumatic causes with disruption of the blood supply. Nontraumatic causes of avascular necrosis may be due to steroid employ, sickle cell disease, or alcoholism among many other etiologies.12 The findings are irregular serpiginous subchondral marrow abnormalities that may progress to collapse of the articular surface (Figure 12-29). The stop-stage of the process is arthritis and joint devastation.
Effigy 12-29. Avascular necrosis. Coronal oblique MRI shows findings of avascular necrosis with subchondral collapse of the medial aspect of the caput (black arrow).
COMMON SURGICAL PROCEDURES/ASSOCIATED COMPLICATIONS
Patients with impingement and instability refractory to conservative management ordinarily undergo subacromial decompression, rotator cuff repair, and repair of glenohumeral instability.13–16
Subacromial decompression is the surgical handling of selection for subacromial impingement. The procedure consists of (1) partial resection of the anterolateral acromion (acromioplasty) and of acromioclavicular osteophytes, (2) coracoacromial ligament resection, and (3) with or without a distal clavicular resection that spares the CC ligaments (Mumford procedure). Normal findings at MRI include remodeling of the acromion, irregularity, or absence of the coracoacromial ligament and widening of the ACJ.
Rotator gage repair may accompany subacromial decompression. Partial tears may be treated arthroscopically. Full-thickness tears usually require an open up procedure. Distal tears are treated by reattachment to the humeral caput, usually to a medialized footprint. More proximal tears are sutured end-to-terminate. Normal findings of the postoperative rotator cuff include balmy thinning, small perforation, and surface irregularity.
The treatment of choice for posttraumatic unidirectional glenohumeral instability is the Bankart procedure. The treatment of option for atraumatic multidirectional glenohumeral instability is the Neer capsular shift process. As has been previously described, posttraumatic instability is ordinarily due to anterior dislocation with associated Bankart and Loma–Sachs lesions. Back-up of the joint capsule is thought to be the cause of multidirectional atraumatic instability.
The Bankart procedure is repair of the Bankart lesion, that is, separation of the inductive inferior labrum from the glenoid. Holes are drilled through the bony glenoid. The inductive junior glenoid labrum is reattached to the os with suture anchors that are passed through the drill holes. Normal findings later the Bankart procedure include fraying/blunting of the labrum, metal artifact at the anterior junior glenoid, and thickening of the joint capsule. An osseous Bankart may be repaired with a screw through the bone fragment.
The Neer capsular shift procedure is a glenohumeral joint capsular tightening process. An incision is made in the anterior joint capsule. The inferior and superior portions of the capsule are shifted to overlap each other. The margins are and so sutured together. Capsular thickening is a normal postoperative finding on MRI.
Operative complications of shoulder surgery include fracture of the acromion, dehiscence of the deltoid, and axillary nerve injury. Chronic postoperative complications include recurrent tears, spiral or suture anchor displacement, and adhesive capsulitis. Recurrent tendon tears manifest as a fluid-filled gap or tendon retraction. Recurrent labral tears depicted equally fluid between the labrum and osseous glenoid or a detached labral fragment.
Imaging of the postoperative is challenging due to artifact from surgical hardware.17 Strategies to subtract artifacts include (1) using long echo train fast spin echo sequences rather than gradient sequences, (2) using STIR rather than frequency-selective fat saturation technique, (3) increasing bandwidth, (4) using a high matrix, and (five) frequency encoding away from area of interest.
Only gilt members can continue reading. Log In or Annals to continue
Source: https://radiologykey.com/shoulder-mri/
0 Response to "How to Read an Mri Report for Shoulder"
Post a Comment